Behavioral Health-Strategic Facility Design Innovations that Improve Treatment Outcomes, Safety and the Bottom Line
On September 17, 2017 in Arlington, Virginia, professionals from across the country came together to expand their knowledge on the current innovations being explored in the world of behavioral health facility design. Attendees represented various fields of practice, including Health Care Facility Managers, Architects, Developers, Interior Designers, Independent Consultants, Researchers, as well as furniture and hardware manufacturers. Seven panel presentations specifically focused on inspiring better-quality care for behavioral health. The experts shared their findings and views in an interactive, collaborative, problem-solving manner, enabling design professionals to expand their physical design strategies and methods to support improved care for behavioral health patients.
The Center for Health Design posed some key questions, which were addressed in each presentation:
“What role can the built environment play in solving the dire and growing mental health and substances abuse crises?”
“What impact do your design decisions have?”
“Are you making use of the best and latest design solutions?”
Based on the presentations I heard, I learned:
Yes, the built environment can play a role in solving the dire and growing mental health and substances abuse crises by integrating design strategies to improve safety with healing environments, and by utilizing the growing body of evidence that helps us understand best practices.
Design decisions have the power to positively (or negatively) impact the outcomes for all parties. Developing the ideal relationships between programmatic functions, and environmental factors is crucial to the decision-making process for patient and staff safety and well-being.
To make the best use of the latest design solutions for creating dignified therapeutic environments it is imperative to be constantly up-to-date with the most recent discoveries and lessons learned. Through continued use of evidence-based design, we are able to continually grow as knowledge-based practitioners.
Design for Mental and Behavioral Health
Presentation #1 – Keynote Speaker
The workshop was initiated by Keynote speaker, Mardelle McCuskey Shepley, of Cornell University, whose presentation was entitled “Design for Mental and Behavioral Health”.
World Bank and the World Health Organization
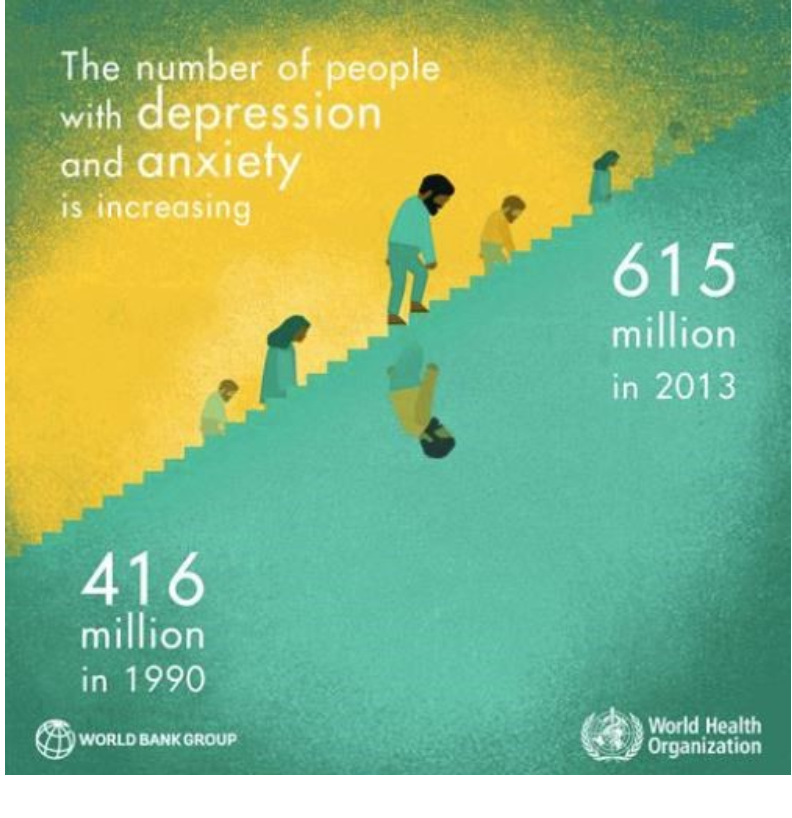
A case for the need to pursue design and research in the realm of Mental Behavioral Health (MBH) environments was made using data from the Substance Abuse and Mental Health Services Administration (SAMHSA) and the World Health Organization (WHO), showing the number of people with depression and anxiety increasing by almost 200 million people over the course of 23 years (1990-2013).
Shepley’s research into critical considerations for facility design exposed a lack of research into MBH Facility design, and the need for informed design strategies that can open doors to dialogue. Supported by the Academy of Architecture for Health, her team presented their findings based on a study aimed at:
Identifying “design features that critically impact staff and patients in MBH Environments; and
Developing “a tool that will evaluate MBH facilities”.
The team identified 17 topics to address staff and patient needs as a result of a review of over 300 sources in 2013, supplemented by a review of over 100 publications in 2017[c1] . (Shepley & Pasha, 2017).
Deinstitutionalization (universally considered a “critical” aspect of MBH environment)
Provision of Maximum Daylight
Private/ Low Density Rooms
Indoor/Outdoor Therapy
Mix of Seating
Patient Staff Interaction/ Observation
Nurse Station design and debate between open and closed stations
Access to Nature visually & physical
Autonomy & Spontaneity
Order & Organization accounting for “Comfortable Complexity”
Well-maintained Environment conveying sense of respect
Damage-resistant & Attractive Furnishings
Social Interaction/ Community
Staff Support &Respite
Suicide Resistant Furnishings
Staff Safety/Security
Smoking Rooms
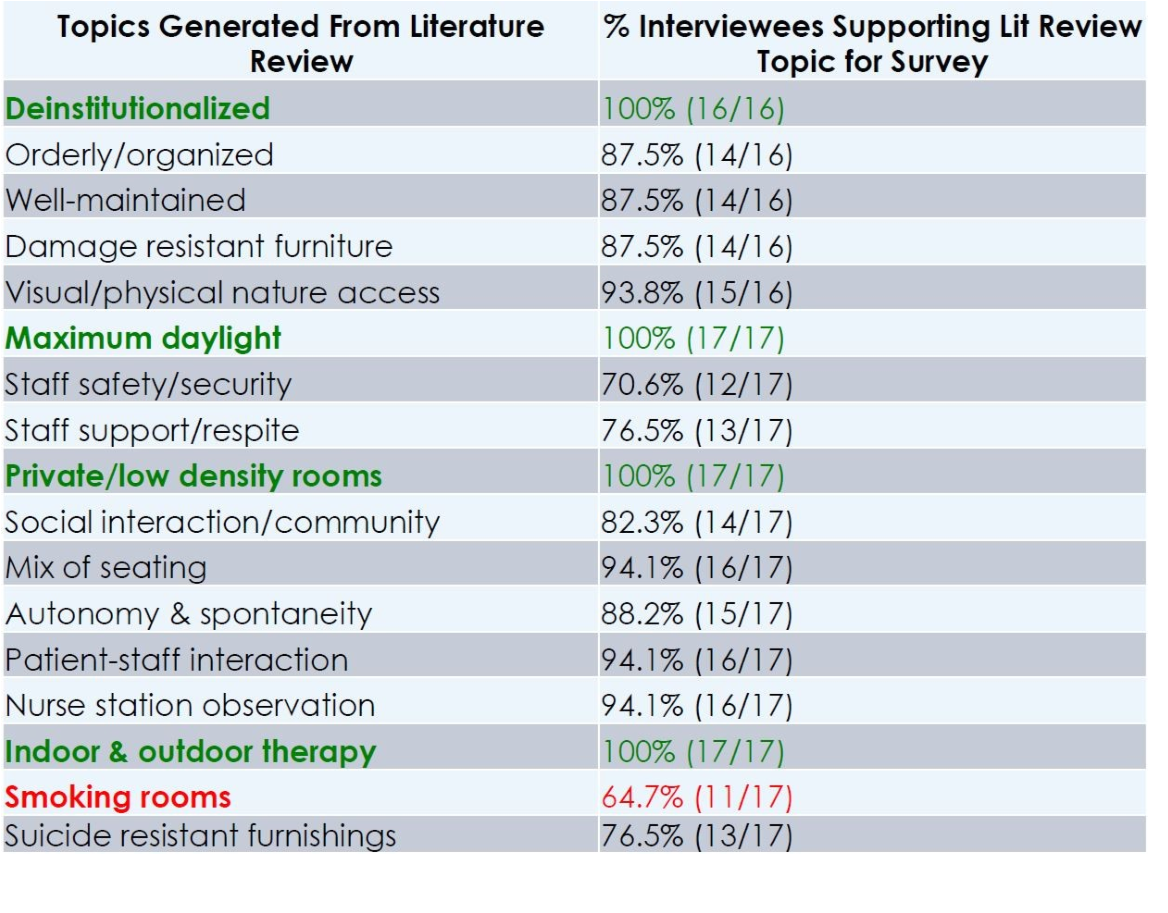
These topics were further explored and investigated through interviews, which were analyzed using the grounded theory method. (Described by Lincoln and Guba, 1985 in Naturalistic Inquiry). The team then rated the importance of these topics, based on the interviews, which revealed that deinstitutionalization, maximum daylight, private/low density rooms, and indoor/ outdoor therapy were 100% supported by interviews as follows:
Retrieved from Environments for Mental & Behavioral Health presentation, by Mardelle McCuskey Shepley, Cornell University, 9/26/17
Each of the above categories collected by Shepley’s team was further expanded on with detailed input and comments from the interviews, such as one interviewee stating that access to nature is “the next great frontier” in the design of mental health facilities. Another point was made that although it is agreed that the provision of natural daylight is critical, it is not always an easy thing to achieve.
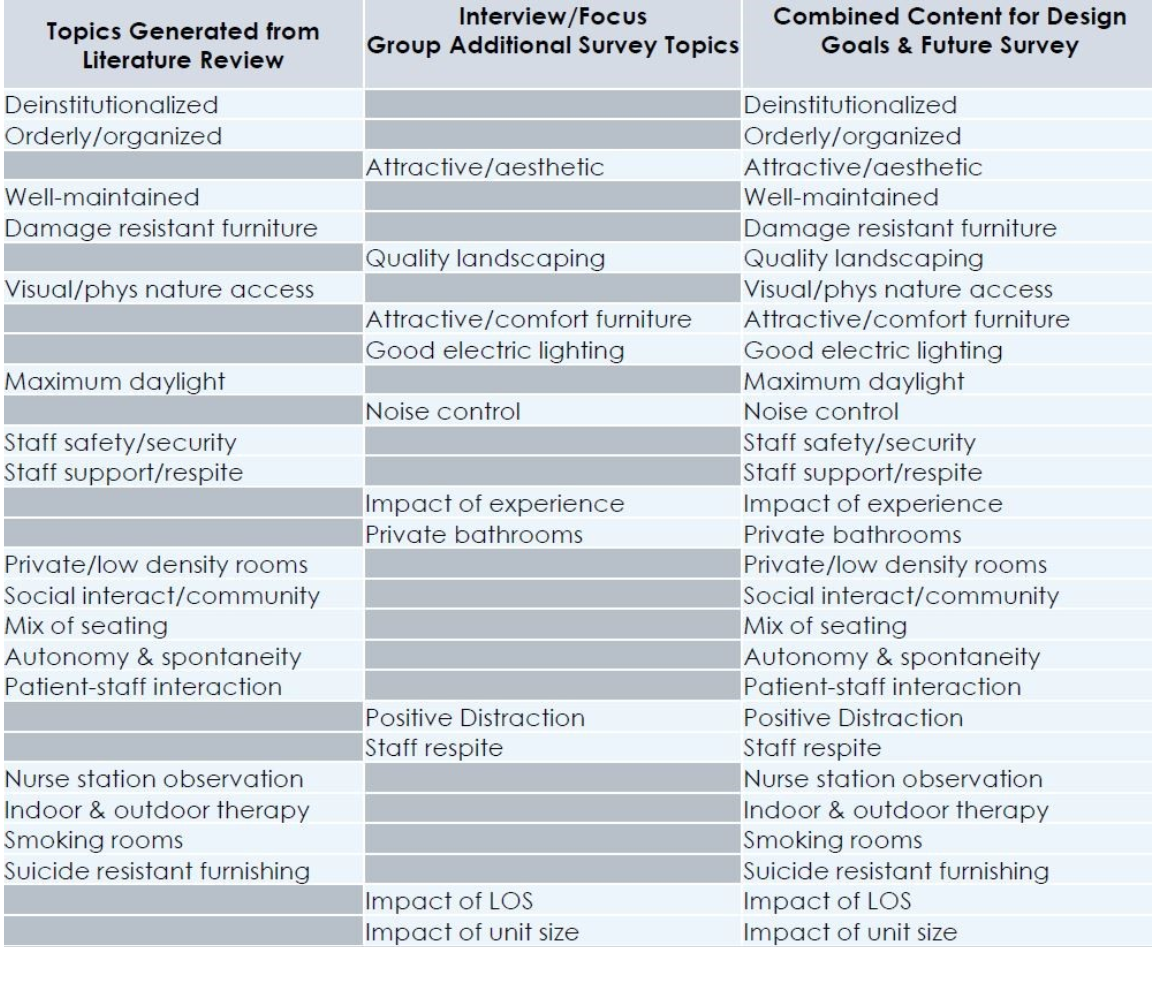
Breaking out the results of the literature review, combined with the interviews, a third category was created, entitled: Combined Content for Design Goals & Future Survey. The matrix from the presentation can be seen below:
Retrieved from Environments for Mental & Behavioral Health presentation, by Mardelle McCuskey Shepley Cornell University, 9/26/17
Using tools such as Psychiatric Staff Environmental Design Surveys (PSED), Shepley’s team studied the importance and effectiveness of these topics, with additional focus on private/semi-private patient rooms and open or closed nursing stations.
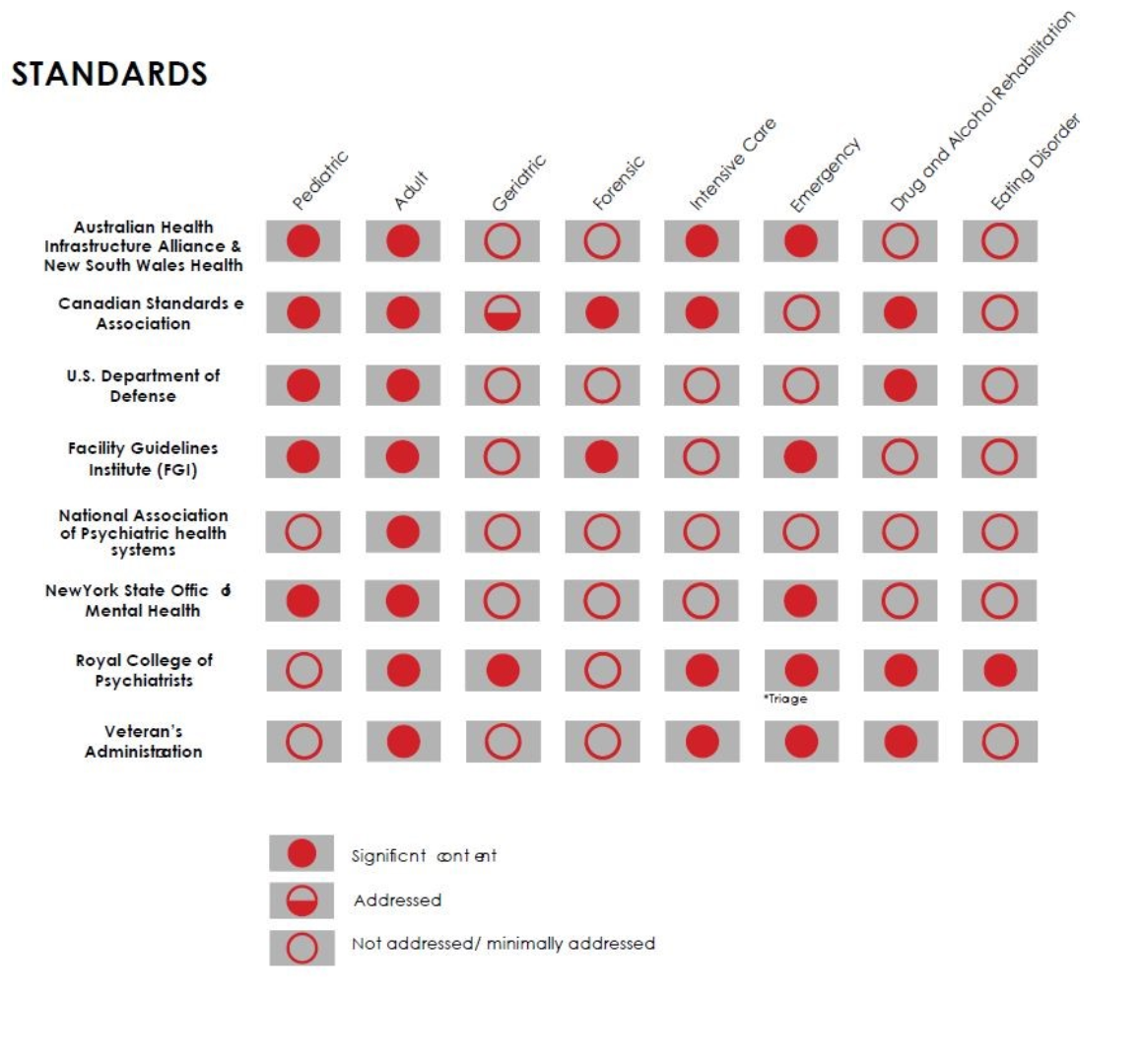
Case studies were shared with diagrams showing integration of design solutions. In addition, Shepley shared a list of industry design standards and the care settings they address. She found that adult mental health environments are most frequently covered in the industry standards, while environments for eating disorder treatment are rarely addressed. The matrix below shows the spaces addressed (and un-covered) in the various industry standards:
Retrieved from Environments for Mental & Behavioral Health presentation, by Mardelle McCuskey Shepley Cornell University, 9/26/17
The lack of attention for behavioral and mental health treatment options is a serious concern. The presenters were hopeful that with developments in genetics, patient participation, guideline development, and public awareness, treatment options will expand. They also suggest that these and changes in social acceptance of mental health disorders will lead to richer, more complex, flexible, and safe mental health spaces.
Making General Hospitals Less Dangerous for Patients with Co-Existing Mental Illness
Presentation #2 - Integrated Inpatient Design
James M. Hunt, AIA and David M. Sine, DrBE, CSP, ARM, CPHRM
Hunt and Sine started their presentation by looking at the history of psychiatric hospitals.
Photo: “Greystone Main Building” by KForce is licensed under CC BY-SA 3.0
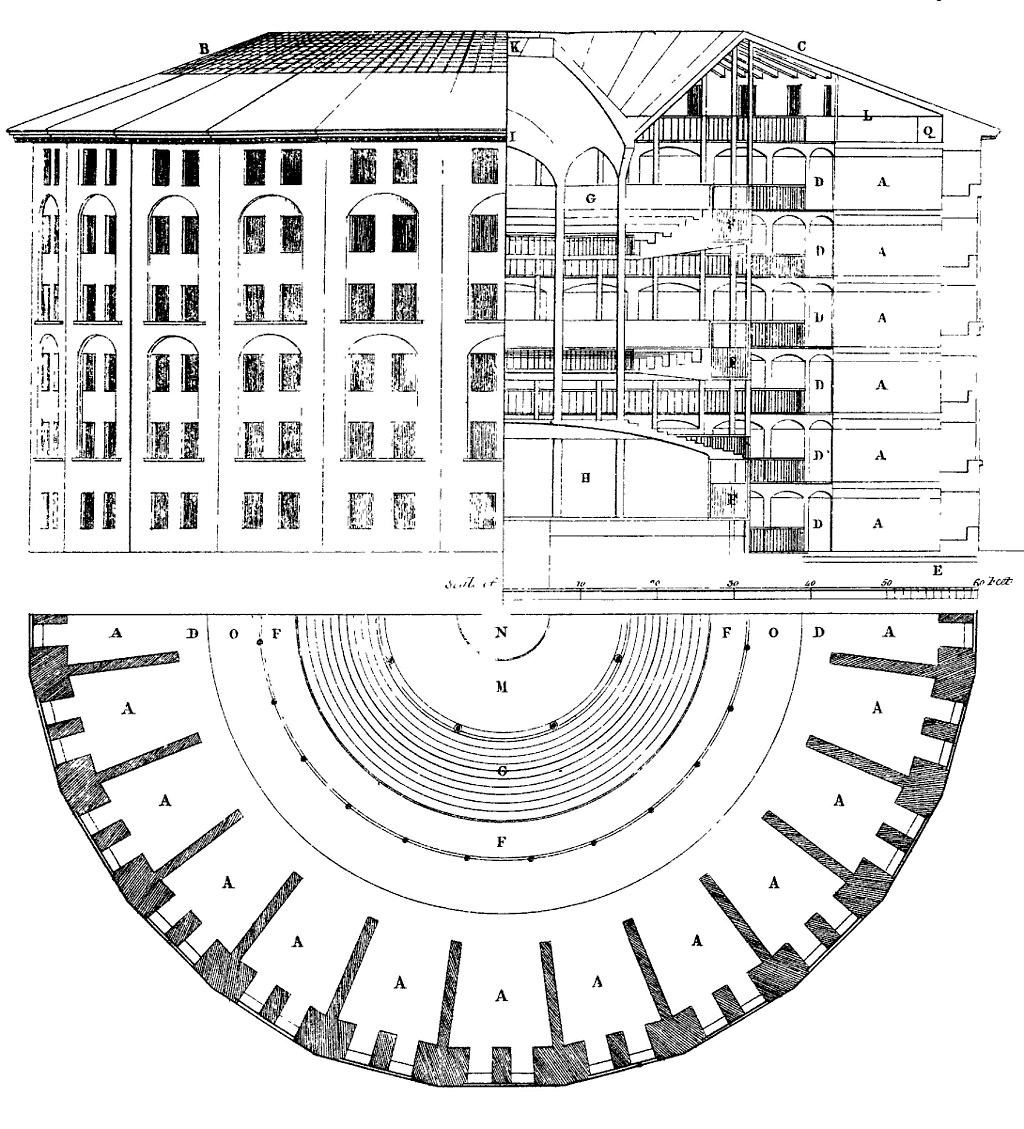
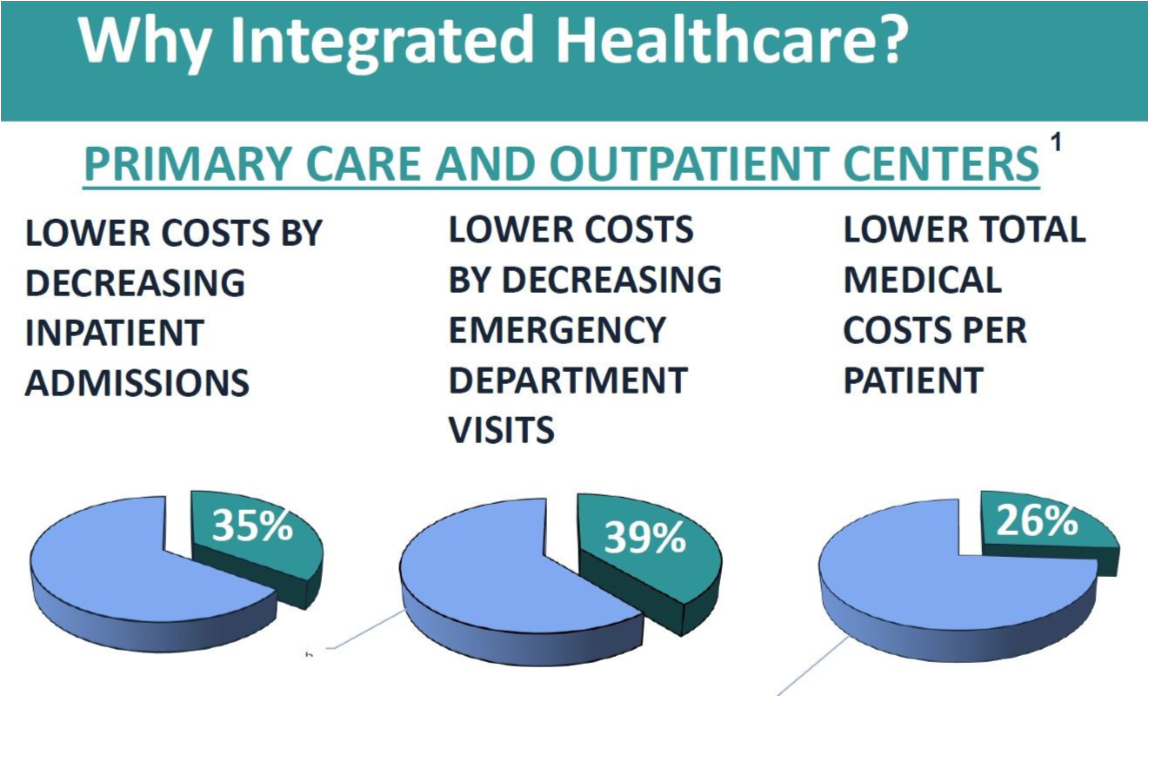
From the famous Greystone Hospital to the Panopticon, to examples of facilities where evidence-based design fell short, resulting in prison-like environments, Hunt and Sine took a stand for “Integrated Healthcare Design”. Their premise was that “treating the whole person (including the diagnoses) in one place by one treatment team is a growing trend that has been “long overdue”.
Source: The works of Jeremy Bentham vol. IV, 172-3, 1843 (originally 1791)
Besides the fact that in their findings “Integrated Healthcare” lowers costs, there is urgency to address medical needs along with mental health needs due to finding that 68% of people with mental illness have one or more chronic physical conditions. This results in a complexity that requires an ability to provide the proper environmental conditions for attending to a patient’s physical and mental healthcare needs, simultaneously. Hunt and Sine spoke about the dangers of patients not getting their medications correctly, because they were being treated for a physical illness, without the doctors being aware of a co-current mental health condition.
Hunt and Sine’s position was that the built environment can help, when designed to minimize access to hazardous items, and when designed with the most consideration possible for minimizing safety risks in patient bedrooms and bathrooms, where most tragedies occur.
Retrieved from Integrated Inpatient Design: Making General Hospitals Less Dangerous for Patients with co-existing Mental Illness presentation, by James M. Hunt, AIA and David M. Sine, DrBE, CSP, ARM, CPHRM, 9/26/17.
As experts and authors of the Facility Guidelines Institute’s (FGI) “Guidelines for the Design and Construction of Hospitals and Outpatient Facilities”, their experience on the subject was shared in detail, emphasizing the importance of the “Safety Risk Assessment”. This combined with The Center for Health Design’s “Safety Risk Assessment Toolkit”, were presented as tools, and fundamentally, requirements for all new construction and remodeling projects.
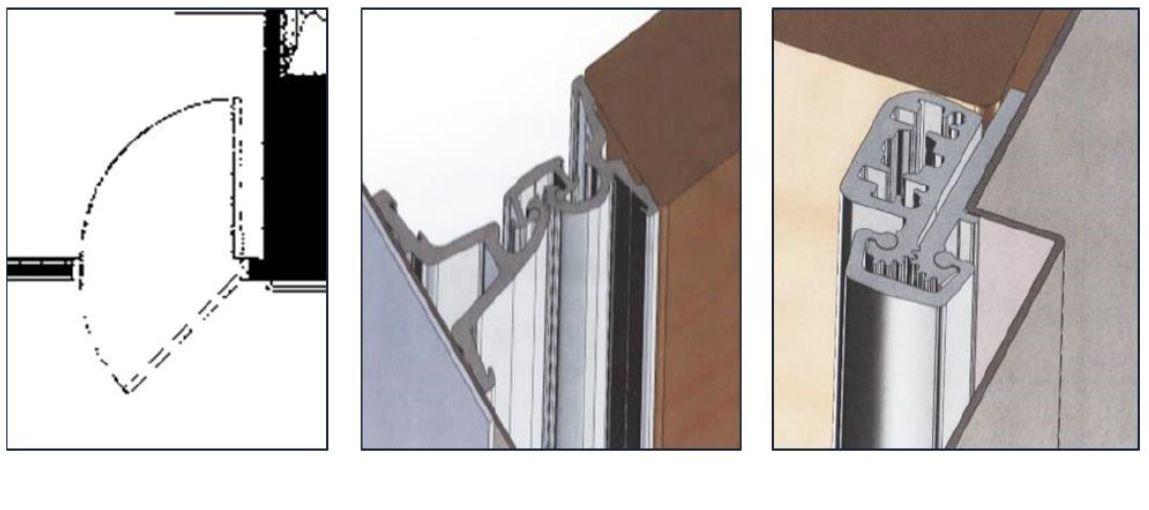
Retrieved from Integrated Inpatient Design: Making General Hospitals Less Dangerous for Patients with co-existing Mental Illness presentation, by James M. Hunt, AIA and David M. Sine, DrBE, CSP, ARM, CPHRM, 9/26/17
The speakers showcased design details for doors, windows, furniture and accessories, that would minimize risk in Med/ Surg facilities.
The summation of their presentation was this quote:
“We must completely rethink almost everything about how we design inpatient rooms and bathrooms, and to consider making every place safe. “ -Hunt & Sine
A Clinic To Address “Invisible” Wounds
Presentation #3 – Wounded Warriors
Tae Y. Jung, AIA, Vice President, Design Leader in NIKA
Fig 1. Screenshot taken from the video Intrepid Spirit Center - TBI Film, by Passing Lane FIlms, 2015. Retrieved 6/12/2018. From: https://vimeo.com/133748504. Screenshot by author.
This impacting presentation dealt with the Invisible Wounds Centers being built for the Department of Defense to treat Veterans, and was specifically focused on designing solutions for those suffering Invisible Wounds of Traumatic Brain Injury (TBI) and Post Traumatic Stress Disorder (PTSD).
“In 2008, the Intrepid Fallen Heroes Fund asked top military and civilian brain specialists to develop a new standard of care for Traumatic Brain Injury. Blending the most advanced findings about the brain with team medicine, we created the Intrepid Spirit Centers.”
-David Hovda, PhD, Director of the UCLA Brain Injury Research Center
Beginning with a video on Intrepid Spirit Centers and TBI, (https://vimeo.com/133748504), the entire audience sat engrossed, some with tears, as testimonies for the efficacy of the Invisible Wound Center programs and clinics were made: Patients spoke about being desperately suicidal and homicidal as a result of three unique PTSD categories of symptoms known as: intrusive, arousal, and avoidant. They spoke of rage at themselves and others, of desperation, and hopelessness - and they spoke of how a clinic, a built environment and physical space, gave them hope and healing.
In the video, Dr. Bret Logan, Director of the Intrepid Center in Fort Campbell, KY, appropriately articulated that Intrepid Spirit Centers are a “Gymnasium for the Brain”.
“From the first minute you walk through the door, you know that this place feels different… that this doesn’t look like any other typical military treatment facility or civilian treatment facility.”
-Captain Rick Freeman, Commanding Officer, US Naval Hospital, Camp Lejeune, NC.
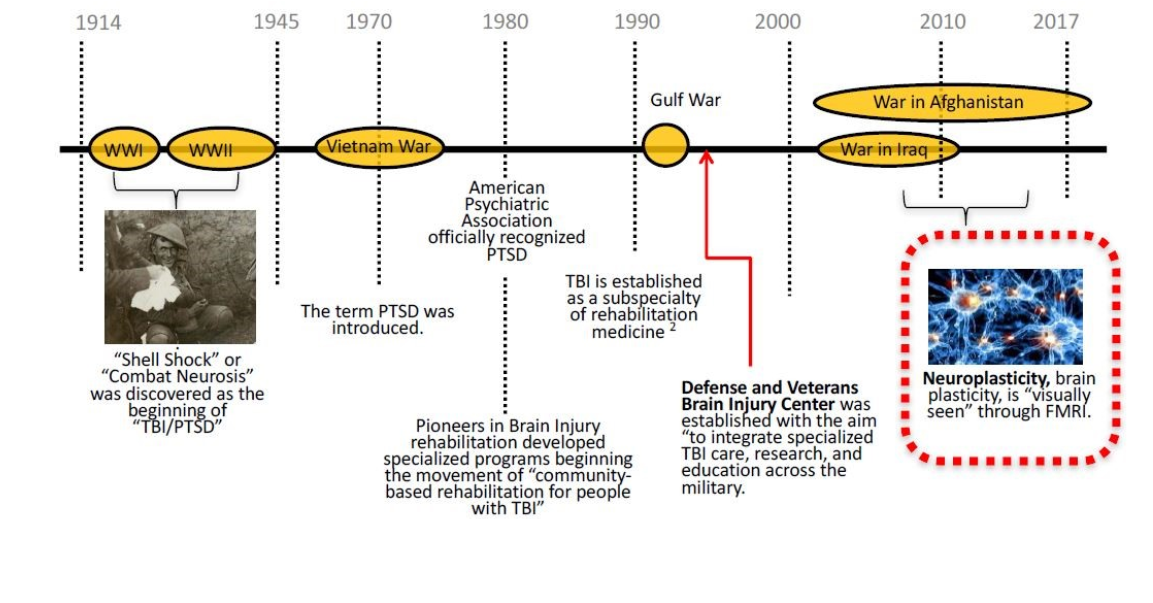
Tae Jung followed up the video with a timeline of TBI/PTSD starting from its identification as “Shell Shock” in 1914 to present day FMRI reports, making brain plasticity (neuroplasticity) visually evident. The developing capacity to study the tremendous potential of neuroplasticity as it is affected by stimulation, negative or positive, has been monumental in assessment of treatments available, and the positive and negative effects of the physical environment.
Retrieved from Invisible Wounds in Military Treatment of TBI/PTSD in DoD Facilities presentation, by Tae Y. Jung, AIA, 9/26/17
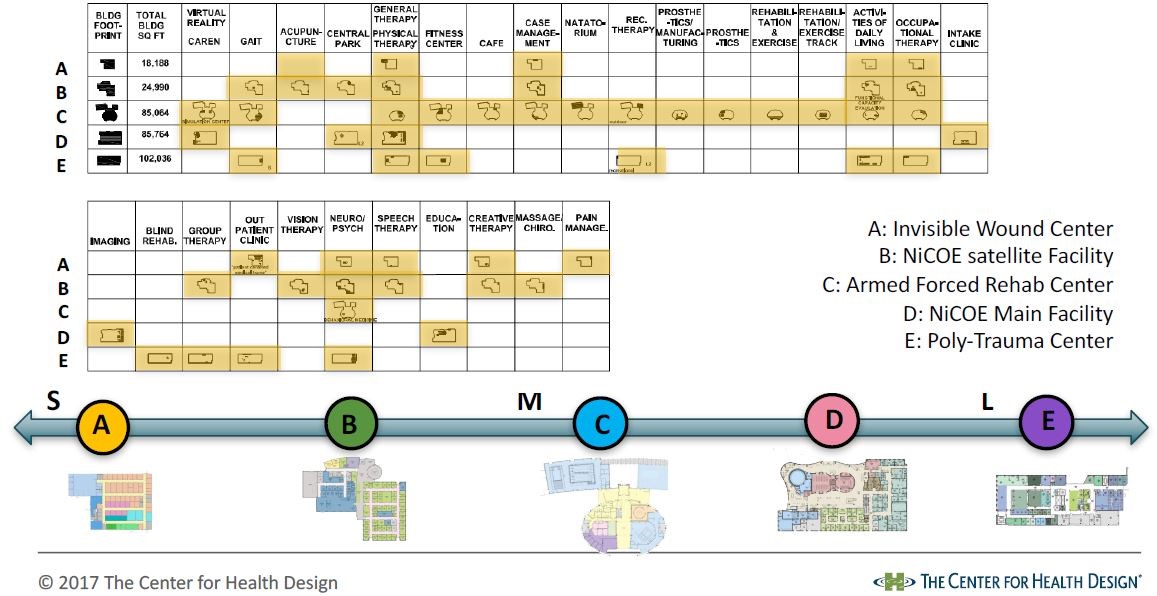
Tae Jung utilized a series of images to diagram the physical, psychological, and neurological manifestations of “Invisible Wounds”. He then presented proposed floor plans, spatial needs, and equipment focused on specific treatment and therapy types in five different military building [c1] types (ranging from 18,188 GSF to 170,000 GSF). The therapy types include:
Acupuncture (Helps activate the body's own self-healing mechanism. It is based on the pattern of energy flow through the body that is essential for health.)
Creative Arts Therapy (Promotes creative expression through art, music, dancing, and writing as outlets to help patients express themselves in new ways and improve their quality of life.)
Physical Therapy (Promotes exercise and physical functioning.)
Occupational Therapy (Promotes training and occupational functioning.)
Recreational Therapy (Provides activities to improve and enhance self-esteem, social skills, motor skills, coordination, endurance, cognitive skills, and leisure skills.)
Prosthetics (Addresses proper wound care and limb management, increases an individual’s strength, flexibility, coordination and endurance, and decreases pain.)
Virtual Reality (Helps people with movement and balance; People navigate through digitally created environments and complete specifically designed tasks often tailored to a treat a specific ailment.)
Neurology (Neuropsychologists focus on thinking skills, behavior, and emotional processing. The NICoE center focuses on diagnosing, treating, and managing conditions of the brain and nervous system.)
Psychology/ Mental Health (A counselor helps a person learn coping skills, how to manage relationships, and improve general emotional well-being.)
Speech Therapy (Focuses on working on a person's ability to form words and other communication skills and how to use special communication devices. Focuses on the muscles in the face, mouth, and throat.)
Retrieved from Invisible Wounds in Military Treatment of TBI/PTSD in DoD Facilities presentation, by Tae Y. Jung, AIA, 9/26/17
Through well-orchestrated and well-balanced treatment that integrates neurology, psychiatric and alternative therapies, combined with the built environment, these clinics have resulted in an amazing success rate of patients dealing with their trauma and neurological functions. These patients are not only able to go back into the world as functioning members of society, but also back into service, which in many cases is very important to them because they have made a commitment to service as their career and calling.
“What’s interesting about it is it takes place in a clinical setting, and it’s not in a research setting, so we know that it works.”
-Dr. Bret Logan, Director, Intrepid Center Fort Campbell, KY
“Located on military bases, Intrepid Spirit Centers are achieving over 90 percent success in returning warfighters to their families and careers.”
-General Richard Cody, Vice Chief of Staff, U.S. Army (2004-2008)
Considering the success of the Defense Centers of Excellence (DCoE) programs, the model they create should seriously be considered for our communities as monumental examples of integrated solution based facilities.
Conclusion
At the end of the workshop, I was full of information and ideas, combined with a reaffirmation that design is making a difference on the lives of children and adults faced with mental health challenges. Architects and designers, in conjunction with user groups, therapists, health care practitioners, and patients are changing how we build for Mental Health.
Fig 2. Screenshot taken from the video Intrepid Spirit Center - TBI Film, by Passing Lane Films, 2015. Retrieved 6/12/2018. From: https://vimeo.com/133748504. Screenshot by author.
This Pebble-In-Practice Workshop was created and hosted by the Center for Health Design: These unique, immersive experiences dive deep into strategic design trends that are shaping tomorrow's healthcare environments. Attendees interact with healthcare industry leaders and colleagues, tour exemplary facilities, and learn through presentations and group think-tanks.
About the Author: Erin Sharp Newton, M. Arch is a part of NK Architects Healthcare Design Group, in Morristown, NJ, advocating for the best possible design outcomes in the area of behavioral health.
Additional Credits
The Center for Health Design (CHD). Natalie Gonzalez (Project Manager, CHD), Ellen Taylor, (Vice President for Research, CHD & Host), SAMHSA, World Health Organization, Watson, Pitts, Garrity, Spelman, Kelkar, Fronsman, Foundation for the Academy of Architecture for Health, Architecture+, Shepley Bulfinch, Pasha, Lincoln, YS. & Guba, EG. (1985). Naturalistic Inquiry. Newbury Park, CA: Sage Publications., Medco., America’s State of Mind; (2010). Available from the internet: http://apps.who.int/medicinedocs/documents/s19032en/s19032en.pdf, Joint Commission. (2007). Suicide Prevention: Toolkit for Implementing National Safety Goal 15A: Joint Commission Resources, The Facility Guidelines Institute, (2014). Guidelines for the Design and Construction of Hospitals and Outpatient Facilities. The Facility Guidelines Institute, 2014, The Center for Health Design. (2015). Safety Risk Assessment Toolkit. Concord, CA: The Center for Health Design. Available from Internet: www.healthdesign.org/insights-solutions/safety-risk-assessment-toolkit-pdf-version, Hunt JM., Sine DM., “Design Guide for the Built Environment of Behavioral Health Facilities –Edition 7.0”. [2015] Facility Guidelines Institute. Available from Internet: http://www.fgiguidelines.org/resource/design-guide-built-environment-behavioral-health-facilities/, NIKA, DoD, Army, Veterans Administration,
The primary goal of this project was to apply the evidence-based design process to inform the design of the new school building. The transdisciplinary team evaluated current research pertaining to the student population, conducted focus groups with staff, and planned a formal study to test hypothesized outcomes in the new space compared to the old space.
The goal of this project was to challenge the aesthetic typically associated with a forensic detention facility and support the client’s healing process by using color to enhance the environment and improve the staff work environment.